
A Brief History and Summary of Stereoscopy in Medicine
written by Lindsay Cole, Canada
Introduction
In life, most humans see the world from two distinct viewpoints: one from each eye. The left eye receives an image slightly different from the right eye because it is focusing on the object of interest from a slightly different angle. The brain uses these differences to perceive depth.
The term ‘Stereoscopy’ refers to what is now more widely known as 3D imaging, i.e., recording and presenting visual information in three dimensions. When a stereoscopic image is viewed properly, the brain perceives depth as it would in the physical world. Thus, a flat paper or screen can carry spatial information. This simple concept can be adapted into drawing, photography and video for true 3D visualization.
Charles Wheatstone discovered the concept of stereoscopy and built the first viewing devices in 18321. By 1852 the Brewster-type stereoscope was publicly available1. This handheld device allowed the common individual to view side-by-side (SBS) stereophotography formats and helped incite the great popularity of stereoscopy in the mid 19th century1. Though this popularity increased and decreased throughout the decades, the concept was continuously applied to a variety of practices including art, film, photography, history, and medicine.
In the present day a variety of viewing devices exist. Polarized light projection and filtered glasses allow both left and right eye images from one screen. It is currently widely used, and known to the general public via 3D movies. SBS stereo images can also be “free-viewed” by those individuals who have trained their eyes to diverge on the page: each eye focused on its corresponding image. This easy access allows the visualization of true 3D depth, as it is naturally perceived by the brain, for a variety of purposes without the need for advanced or expensive technologies.
Stereoscopy in Medical Education
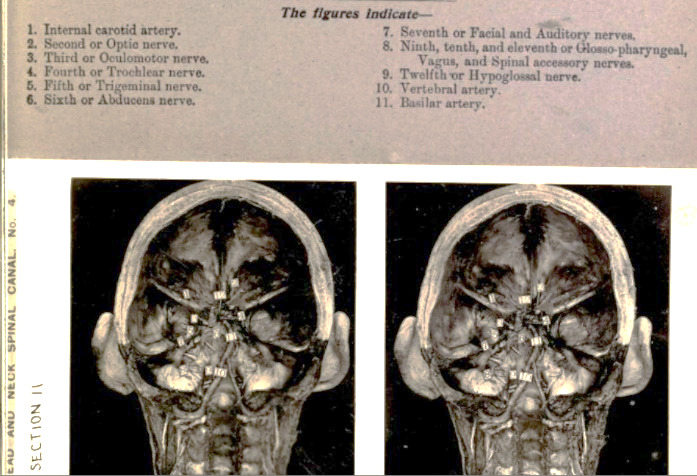
The use of stereoscopy for medical education began in the early 20th century. Some sources indicate that Dr. Daniel John Cunningham was the first to use SBS stereographs to teach human anatomy2,3. In 1909 his work was compiled into several volumes of Stereoscopic Studies of Anatomy, eventually comprising the Edinburgh Stereoscopic Atlas of Anatomy3,4. By the mid-century mark, a resurgence in the popularity of stereoscopic viewing sparked collaboration between anatomist Dr. David L. Bassett and William B. Gruber, inventor of the Viewmaster system. They created a collection of stereoscopic disks featuring dissections by Bassett and photographs by Gruber: A Stereoscopic Atlas of Human Anatomy4.
Stereoscopic anatomical teaching continues to be of use today. The retention of knowledge in medical student groups shown 3D stereoscopic videos is greater than that of groups shown 2D videos2,6. This result is significant in anatomical relationships, while functional knowledge appears unaffected2. The strength of this learning impact is still unknown. Some studies determined no significant difference in written test scores between 3D and 2D video learning7. These inconclusive results are potentially due to the type (ie. functional verses spatial) of questions tested. The benefit of 3D learning varies from person to person. A large predictor of a student’s success in anatomic learning is visuospatial ability; stereoscopic learning aids may be more beneficial for those with lower natural visuospatial scores6,7,8. It effectively evens the playing field. Unfortunately, though many medical schools currently give students access to 3D computer models, they are displayed or projected onto flat screens, and thus lose the actual stereoscopic benefit6,8. Modern teaching programs with true stereoscopic projection of CT vascular models have been introduced through polarized projection7,9. When introduced to stereoscopic techniques of learning, students find it useful and are interested in using it in the future6,10.
Figure 1: Stereoscopic teaching tools throughout the decades (1905–1960).
In the 21st century, stereoscopic teaching has been thoroughly modernized and adapted, significantly in the field of neurosurgery, where many practice-hours are needed despite limited availability of patients and OR time10. Virtual reality (VR) simulations in 3D space allow residents to gain experience in the field without risk to patients10. These can be both haptic (touch simulation) and non-haptic, and studies have shown them to be significantly beneficial compared to control groups without VR, though some uncertainty exists11,12,13. The hepatic portion of the simulation training may not contribute significantly to the benefit, suggesting that the improved learning outcomes is due to the stereoscopic VR13. Stereoscopic models are also used for learning purposes in other specialities10.
Stereoscopy in Surgery
Stereoscopic techniques in surgery are not simply limited to training and simulation. As early as 1922, surgeons had adapted the knowledge of stereopsis for use in the OR15. Gunnar Holmgren retained depth when magnification was required by first using binocular microscopes at the University Clinic of Stockholm15. This technique was quickly employed worldwide and had especial benefit in the small surgeries of the head and neck15.
Stereoscopy is also a useful phenomenon in laparoscopic surgeries. Traditionally, the laparoscope video is displayed on a 2D monitor and therefore lacks potentially crucial depth information. Stereoscopic laparoscopes allow true 3D relationships to be determined without opening the body cavity to human eyes16. This is done simply by including two visual viewpoints and then viewing them via any stereoscopic method. As minimally invasive surgeries, and therefore laparoscopy, increased in complexity, the difficulties of performing procedures without depth became apparent17. In the early 1990s stereoscopic laparoscopy was used for the first time on human patients: a laparoscopic cholecystectomy performed at Nuclear Research Center Karlsruhe17. The incorporation of stereoscopy in laparoscopic procedures increases the ease of tasks that require 3D visualization such as organ mobilization and suturing17. A 2017 literature review by Schwab et al. collected objective and subjective information from patients and surgeons using 2D vs 3D laparoscopic systems during cholecystectomy operations18. They found that there were no increased negative outcomes in either method, and that many surgeons perceived better depth perception and control with the 3D systems18. Stereoscopic laparoscopy can also be combined with laparoscopic ultrasound for augmented reality views of internal structures16.
Image-guided surgery (IGS) is widely used in a variety of fields14. IGS allows a 3D surgical plan to be developed on a 3D model of the patient which is created from preoperative imaging14. 3D models are also used for pre-planning, head frame placement and to determine accessibility before radiosurgery19. This shortens procedure times, optimizes patient experience and decreases repeat procedures19. Unfortunately, most of these models are viewed on a 2D monitor, eliminating the benefit of true stereoscopic effect14. It would be beneficial and feasible to include stereoscopic viewing through a polarized display14.
3D imaging can be performed intraoperatively within the OR through stereoscopic recording and polarization14. These images may be combined with the preoperative models for intraoperative visualization14. The ease of incorporating stereoscopy into surgery increases as technology develops. Something as commonly available as a smartphone can be adapted into a viewing device20. Successful robot-assisted ophthalmic surgery simulations have been performed by attaching a stereoscopic camera to a binocular surgical microscope and displaying the resultant image on a smartphone VR headset20.
High-definition stereoscopic 3D imaging in real-time is crucial in the emerging field of telesurgery. With ultra-fast 5G internet connection it is possible to perform robot-assisted laparoscopic surgeries thousands of kilometres from the patient site21,22. These methods, though still new, could potentially combat surgeon shortages, remote access problems, and disease spread21.
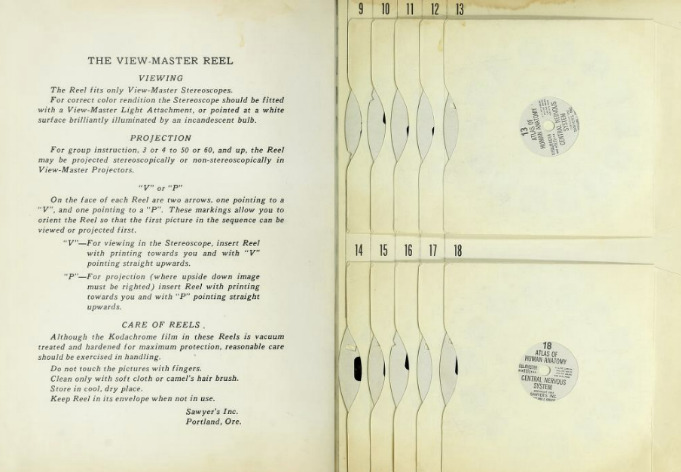
Figure 2: An example of telesurgery technologies.
Left: The surgeon console contains a stereoscopic image viewer and mobile master manipulators to control the patient side cart.
Right: The patient side cart performs the robot-assisted surgery via commands from the surgeon console.
Stereoscopy in Ophthalmology
Stereoscopy is an important part of vision. Screening and testing for stereoscopic acuity can help diagnose a variety of ocular conditions including strabismus and amblyopia23. There are several stereoscopic tests ranging in specificity and ease of use for the appropriate patient case and physician concern.
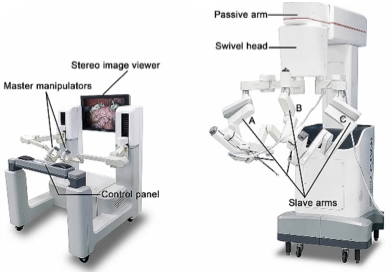
In 1960 Bela Julesz used random-dot stereocards to test for stereoscopic acuity23. These random patterns of dots appear flat and uninteresting when viewed monocularly, but when the test subject uses intact binocular vision through a stereoscopic viewing device, shapes emerge in the depth23. The TNO stereotest utilizes the same concept and tests mostly for amblyopia23. It is viewed in red/blue anaglyph and consists of recognisable images instead of depth clues23. TNO tests are designed so that when viewing monocularly, an incorrect image is still visible23. A quantitative aspect is also added23. The Lang test is similar again, but uses a panographic viewing technique where no special glasses are required23. The most common stereotest is the Titmus test, in which raised shapes and objects are detected when viewed through polarized glasses23.
Lang’s two pencil test, first described in 1983, removes the need for any specialized stereodevice24. It requires that the patient correctly line up a pencil with one held by the examiner; binocular performance is compared against monocular in each eye23,24,25. This is a qualitative test and is not used for diagnosis, but has been shown to distinguish gross strabismus at a high sensitivity and specificity compared to random-dot and TNO with a negative predictive value of 100%25.
Figure 3: Stereoscopic acuity tests.


Stereoscopy is not only used to test for ocular conditions; it’s also used to treat them. Non-surgical treatments of eye movement and ocular muscle disorders such as strabismus are known as orthoptics: these include stereoscopic exercises. Dr. Louis Javal introduced orthoptic treatment for strabismus in the late 19th century, using early Wheatstone stereoscopes to induce proper binocular focus26. The binocular training provided by these treatments is used in replacement of and to support surgery26. The over-reliance and misuse of early orthoptics damaged their therapeutic reputation around the turn of the century, but treatments were modernized in 1919 by doctors E. E. and M. C. Maddox and eventually re-popularized their use26. M. C. Maddox created stereocards for the amblyoscope (later the synoptophore), a reflecting stereoscope-like device that allows for individual eye stimulation with lights, divergence angle measurement, and determination of the area of suppression27.
In 1927 Dr. Carl Sattler published the first set of orthoptic stereocards for strabismus diagnosis and treatment that were available for use at home28. They were inexpensive and available for parents to purchase for their children28. Other similar sets were soon available and widely used until the 1950s28.
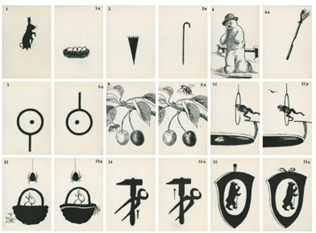
Figure 4: Orthoptic stereocards for strabismus diagnosis and treatment.
The benefit of orthoptic exercises continues to be of controversy today. Ophthalmologists dispute whether lengthy exercises support marked therapeutic improvement26. Studies have shown that stereoscopic orthoptic training for only two weeks (15 mins twice a day) mildly increases the angle of fusion in strabismus patients and decreases the required prismatic correction29. Longer training can lead to greater improvement and the remission of tropia29. These benefits depend on the individual’s motivation, time commitment, and the nature of their presenting strabismus29,30. Exodeviation seems to benefit more than esodeviation, while vertical deviation shows no effect29. The outcome of orthoptic training depends largely on the severity of strabismus prior to starting therapy: better results correlate with milder cases30. Non-surgical treatments are therefore reserved for mild or small angle strabismus26,29,30. They cannot overcome large disparities that would benefit from surgery26. These inherent limitations of orthoptics are often misunderstood, leading to misapplication of orthoptic therapies, poor outcomes and decreased clinical support26.
Stereoscopy can also be used in screening for glaucoma31. Ocular fundus images are often analyzed for diagnostic characteristics of the optic nerve head; this is especially true for normotensive glaucoma that cannot be detected with a tonometer31. Important features such as the cup depth, disc shape and cup to disc ratio are used in screening31,32. Correct diagnosis of glaucoma based on these features is aided by stereoscopic analysis31,32,33,34. Ophthalmologists can view these stereoscopic images either digitally or on film33. When comparing glaucoma detection using stereoscopic versus monoscopic images, the stereoscopic screening detects cases at increased sensitivity and reproducability32. Stereoscopic images more accurately indicate glaucoma patients that are nearer the cup to disc ratio threshold32. Furthermore, computer-aided machine-learning detection methods that focus on analyzing stereoscopic images of the ocular fundus outperform those that rely only on a single image with no depth information31,34.
Conclusion
This is by no means a comprehensive collection of the uses of stereoscopy in medicine. The increased information of 3D contributes benefits to many areas of imaging not mentioned above, such as screening mammography, echocardiography, bronchoscopy and scintigraphy35,36,37,38. Humans exist in and process the physical world in three dimensions; it is no surprise that the best medical observations also include depth information.
Stereoscopy remains a long-studied and under-used technology in medicine. It is used widely in some specialities, including anatomy, neurosurgery, laparoscopic surgery, imaging and ophthalmology, but remains a relatively unknown concept in the general medical and non-medical population. Common criticisms of stereoscopy in all fields include the need for additional viewing devices, glasses or tools10,23,32. While this is potentially true, novel and inexpensive stereoscopic devices are available in the majority of cases20,28.
The popularity of stereoscopy has ebbed and flowed over the many decades since Charles Wheatstone first described its principle1. The extent of its use in medicine has followed a similar process. The current progress in computer technology allows for increased consumption of modern 3D movies, and increased innovation in the medical field. We exist in a current stereoscopic boom. There are more opportunities for stereoscopy in virtual care and remote procedures21,22. More 3D tools are available to medical students6,8. For recorded depth information to be of benefit, 3D data need to be viewed not from flat screens, but from stereoscopic viewers. Only in this way is the patient truly represented.
Acknowledgements
Thank you to Andrew Lauren for editing, proofreading and contributing from his wonderful collection! Thanks also to David Kuntz and Brian May for directing my areas of focus.
Abbreviations
2D Two dimensional
3D Three dimensional
SBS Side-by-side (stereoscopic viewing)
OR Operating room
VR Virtual reality
CTA Computed tomographic angiogram
IGS Image-guided surgery
References
- Pellerin D. Stereoscopy: The Dawn of 3D. May BH, editor. London: London Stereoscopic Company; 2021.
- Bernard F, Richard P, Kahn A, Fournier HD. Does 3D stereoscopy support anatomical education? Surg Radiol Anat. 2020 Jul;42(7):843–852. doi: 10.1007/s00276-020–02465‑z. Epub 2020 Apr 4. PMID: 32248256.
- Cunningham DJ. Stereoscopic studies of anatomy, vol 3. New York: Imperial Publishing Company; 1911.
- Cunningham DJ. Stereoscopic studies of anatomy, vol 2. New York: Imperial Publishing Company; 1909.
- Bassett DL. A Stereoscopic Atlas of Human Anatomy. Portland, Oregon: Sawyer’s Inc.; 1962.
- Cui D, Wilson TD, Rockhold RW, Lehman MN, Lynch JC. Evaluation of the effectiveness of 3D vascular stereoscopic models in anatomy instruction for first year medical students. Anatomical Sciences Edu. 2016 Jun;10(1):34–45. doi: 10.1002/ase.1626
- Goodarzi A, Monti S, Lee D, Girgis F. Effect of Stereoscopic Anaglyphic 3‑Dimensional Video Didactics on Learning Neuroanatomy. World Neurosurg. 2017 Nov;107:35–39. doi: 10.1016/j.wneu.2017.07.119. Epub 2017 Jul 29. PMID: 28765017.
- Luursema JM, Verwey WB, Kommers PAM, Annema JH. The role of stereopsis in virtual anatomical learning. Interacting with Computers. 2008 Sep;20(4–5):455–460. doi: 10.1016/j.intcom.2008.04.003
- Cui D, Lynch JC, Smith AD, Wilson TD, Lehman MN. Stereoscopic vascular models of the head and neck: A computed tomography angiography visualization. Anat Sci Educ. 2016 Mar-Apr;9(2):179–85. doi: 10.1002/ase.1537. Epub 2015 Apr 30. PMID: 25929248.
- Jacquesson T, Simon E, Dauleac C, Margueron L, Robinson P, Mertens P. Stereoscopic three-dimensional visualization: interest for neuroanatomy teaching in medical school. Surg Radiol Anat. 2020 Jun;42(6):719–727. doi: 10.1007/s00276-020–02442‑6. Epub 2020 Feb 29. PMID: 32114650.
- Rolland JP, Wright DL, Kancherla AR. Towards a novel augmented-reality tool to visualize dynamic 3‑D anatomy. Stud Health Technol Inform. 1997;39:337–48. PMID: 10168929.
- Unger B, Tordon B, Pisa J, Hochman JB. Importance of Stereoscopy in Haptic Training of Novice Temporal Bone Surgery. Stud Health Technol Inform. 2016;220:439–45. PMID: 27046619.
- Erolin C, Lamb C, Soames R, Wilkinson C. Does Virtual Haptic Dissection Improve Student Learning? A Multi-Year Comparative Study. Stud Health Technol Inform. 2016;220:110–7. PMID: 27046562.
- Christopher LA, William AMS, Cohen-Gadol AA. Future Directions in 3‑Dimensional Imaging and Neurosurgery Stereoscopy and Autostereoscopy. Neurosurg. 2013;72:A131-A138. doi: 10.1227/NEU.0b013e318270d9c0
- Uluç K, Kujoth GC, Başkaya MK. Operating microscopes: past, present, and future. Neurosurg Focus. 2009;27:E4. doi: 10.3171/2009.6.FOCUS09120
- Kang X, Azizian M, Wilson E, Wu K, Martin AD, Kane TD, Peters CA, Cleary K, Shekhar R. Stereoscopic augmented reality for laparoscopic surgery. Surg Endosc. 2014 Jul;28(7):2227–35. doi: 10.1007/s00464-014‑3433‑x. Epub 2014 Feb 1. PMID: 24488352.
- Becker H, Melzer A, Schurr MO, Buess G. 3‑D video techniques in endoscopic surgery. Endosc Surg Allied Technol. 1993 Feb;1(1):40–6. PMID: 8050009.
- Schwab K, Smith R, Brown V, Whyte M, Jourdan I. Evolution of stereoscopic imaging in surgery and recent advances. World J Gastrointest Endosc. 2017 Aug 16;9(8):368–377. doi: 10.4253/wjge.v9.i8.368. PMID: 28874957; PMCID: PMC5565502.
- Ford E, Purger D, Tryggestad E, McNutt T, Christodouleas J, Rigamonti D, Shokek O, Won S, Zhou J, Lim M, Wong J, Kleinberg L. A virtual frame system for stereotactic radiosurgery planning. Int J Radiat Oncol Biol Phys. 2008 Nov 15;72(4):1244–9. doi: 10.1016/j.ijrobp.2008.06.1934. PMID: 18954719.
- Ho DK. Using smartphone-delivered stereoscopic vision in microsurgery: a feasibility study. Eye (Lond). 2019 Jun;33(6):953–956. doi: 10.1038/s41433-019‑0356‑8. Epub 2019 Feb 12. PMID: 30755728; PMCID: PMC6707160.
- Mohan A, Wara UU, Arshad Shaikh MT, Rahman RM, Zaidi ZA. Telesurgery and Robotics: An Improved and Efficient Era. Cureus. 2021 Mar 26;13(3):e14124. doi: 10.7759/cureus.14124. PMID: 33927932; PMCID: PMC8075759.
- Zheng J, Wang Y, Zhang J, Guo W, Yang X, Luo L, Jiao W, Hu X, Yu Z, Wang C, Zhu L, Yang Z, Zhang M, Xie F, Jia Y, Li B, Li Z, Dong Q, Niu H. 5G ultra-remote robot-assisted laparoscopic surgery in China. Surg Endosc. 2020 Nov;34(11):5172–5180. doi: 10.1007/s00464-020–07823‑x. Epub 2020 Jul 22. PMID: 32700149.
- Pateras E, Plakitsi A, Chatzipantelis A. Stereoscopic Vision & Testing Techniques – Overview. Biomed. J. Scientific and Technical Res. 2020 Mar;26(5):20252–20260. doi: 10.26717/BJSTR.2020.26.004405
- Lang J. Der Treffversuch zur Prüfung des Stereosehens [The two-pencil test for testing stereopsis]. Klin Monbl Augenheilkd. 1983 Jun;182(6):576–81. German. doi: 10.1055/s‑2008–1054858. PMID: 6876657.
- Nongpuir ME, Sharma P. Horizontal Lang two-pencil test as a screening test for stereopsis and binocularity. Indian Journal of Ophthalmology 58(4):287–90. doi: 10.4103/0301–4738.64125
- Parks MM. Strabismus care: Past, present and future. Doc Opthalmol. 1973 Feb;34:301–315. doi: 10.1007/BF00151817
- Synoptophore (Major Amblyoscope) Information Guide. HS Clement Clarke Opthalmic. Harlow, Essex: Haag-Streit UK; Nov 2014.
- Landecker H. What do you see?. Hidden Treasure: The National Library of Medicine. New York: Blast Books; 2011
- Borowiec-Wojtanowska A, Baranowska-George T. Leczenie chorych z małym katem zeza ćwiczeniami na telestereoskopie Starkiewicza i synoptoforze [Treatment of patients with small angle squint by exercising with Starkiewicz’s tele-stereoscopy and synoptophore]. Klin Oczna. 1994 Jun-Jul;96(6–7):197–9. Polish. PMID: 7897972.
- Goldrich SG. Optometric therapy of divergence excess strabismus. Am J Optom Physiol Opt. 1980 Jan;57(1):7–14. doi: 10.1097/00006324–198001000-00002. PMID: 7377279.
- Liu Y, Yip LWL, Zheng Y, Wang L. Glaucoma screening using an attention-guided stereo ensemble network. Methods. 2021 Jun 19:S1046-2023(21)00162–6. doi: 10.1016/j.ymeth.2021.06.010. Epub ahead of print. PMID: 34153436.
- Shrestha R, Budenz DL, Mwanza JC, Tulenko SE, Fleischman D, Gower EW. Comparison of vertical cup-to-disc ratio estimates using stereoscopic and monoscopic cameras. Eye (Lond). 2021 Dec;35(12):3318–3324. doi: 10.1038/s41433-021–01395‑3. Epub 2021 Jan 29. PMID: 33514892; PMCID: PMC8602644.
- Hasanreisoglu M, Priel E, Naveh L, Lusky M, Weinberger D, Benjamini Y, Gaton DD. Digital versus film stereo-photography for assessment of the optic nerve head in glaucoma and glaucoma suspect patients. J Glaucoma. 2013 Mar;22(3):238–42. doi: 10.1097/IJG.0b013e31823298da. PMID: 21946551.
- Norouzifard M, Dawda A, Abdul-Rahman A, GholamHosseini H, Klette R. Superpixel segmentaion methods on stereo fundus images and disparity map for glaucoma detection. 2018 International Conference on Image and Vision Computing New Zealand (IVCNZ). 2018 Nov:1–6. doi: 10.1109/IVCNZ.2018.8634732.
- Ferre R, Goumot PA, Mesurolle B. Stereoscopic digital mammogram: Usefulness in daily practice. J Gynecol Obstet Hum Reprod. 2018 Jun;47(6):231–236. doi: 10.1016/j.jogoh.2018.03.009. Epub 2018 Apr 3. PMID: 29621618.
- Harake D, Gnanappa GK, Alvarez SGV, Whittle A, Punithakumar K, Boechler P, Noga M, Khoo NS. Stereoscopic Display Is Superior to Conventional Display for Three-Dimensional Echocardiography of Congenital Heart Anatomy. J Am Soc Echocardiogr. 2020 Nov;33(11):1297–1305. doi: 10.1016/j.echo.2020.06.016. Epub 2020 Sep 9. PMID: 32919855.
- Nobuyama S, Sato T, Handa H, Nishine H, Inoue T, Mineshita M, Miyazawa T. Comparison of Airway Measurements for Tracheobronchial Stenosis Between Stereoscopic Bronchoscope and MD-CT. J Bronchology Interv Pulmonol. 2017 Oct;24(4):296–302. doi: 10.1097/LBR.0000000000000409. PMID: 28957890.
- Tanaka C, Fujii H, Ikeda T, Jinno H, Nakahara T, Suzuki T, Kitagawa Y, Kitajima M, Ando Y, Kubo A. Stereoscopic scintigraphic imaging of breast cancer sentinel lymph nodes. Breast Cancer. 2007;14(1):92–9. doi: 10.2325/jbcs.14.92. PMID: 17245002.
Lindsay Cole (Victoria, Canada)
My stereo-hobby is quickly approaching its 3rd birthday, proving once again how time flies! I started taking stereo photos when I was living in Hamburg, Germany, and needed a personal interest to pass the time. Like many people I first encountered the stereo process thanks to Dr. Brian May, and since then I’ve met many wonderful photographers and artists! I mainly enjoy hyperstereos and photos that can demonstrate the grandiosity of my subjects. Having returned to Canada, my main focus has been the natural beauty and colour that surrounds me every day. Any time I’m on a hike or camping excursion I’m sure to snap a few pictures! It’s amazing how much you can do with a smartphone. My only equipment currently is my trusty, old, cracked Samsung Note 8… the camera is great and that’s all that matters! Sequential photos do have a limit, but there’s enough for me to work with for now!
Instagram-profile: staring.at.stereos